
Reflections on the Incel Talk by the Connecting Psychology Hub
Today, I want to share my reflections on the insightful talk about incels, hosted by the Connecting Psychology Hub. Walking in, I had no idea what the term “incel” actually meant. I attended out of curiosity and a genuine desire to understand how this concept might relate to our psychological work. I anticipated learning something interesting—but I left with far more than expected.
What Are Incels?
We began by unpacking the term “incel”, short for “involuntary celibate”. Initially, it was coined from a social justice perspective to support people who, despite wanting romantic or sexual relationships, struggle to form them. It was meant to be a compassionate label—one that acknowledged a difficult experience and created a sense of community.
The incel community began between 1993 and 1997 with Alana’s Involuntary Celibacy Project. This created by a Alana seeking to understand and connect with others experiencing romantic loneliness. It was intended as a compassionate, inclusive space for people of all genders who struggled with forming intimate relationships despite desiring connection and companionship. By the early 2000s, the community began to drift toward pessimism. From 2005 to 2013, it embraced blackpill philosophy and isolation. In 2014, Elliot Rodger became a catalyst for more radical changes. Between 2015 and 2017, fragmentation and radicalisation increased, leading to global attention in 2018 after Alek Minassian's attack. From 2019 to 2022, the culture deepened through memeification and echo chambers. Most recently, from 2023 to 2025, the trend appears to show quiet persistence and subtle adaptation.
Over time, however, the term has been adopted by certain online subcultures, shifting its original purpose. Many of these spaces now serve as echo chambers that promote exclusion, alienation, and sometimes, deeply misogynistic or fatalistic ideologies.
The Internet as Identity Space
A key insight from the talk was the concept of internet identity. Rather than seeing the internet as just a platform, we explored it as a space—akin to physical communities—where individuals form and express evolving identities. Terms like digital natives, digital immigrants, and digital nomads help us understand the nuances of people’s engagement with digital spaces.
This understanding is especially crucial when reflecting on the incel identity. Though it is not a clinical diagnosis, it is undeniably a social identity—one that powerfully influences mental health. Using social identity theory, we can see how such identification may lead to increased anger, low self-worth, and isolation, all of which reinforce barriers to seeking connection or professional help.
Mental Health and Employment
The talk shed light on troubling mental health patterns among incels. Research suggests those identifying with the label often face elevated rates of suicidality, depression and anxiety, as well as higher prevalence of autism spectrum conditions and ADHD. These individuals may also experience severe self-criticism and chronic feelings of rejection.
We also examined the ideologies of the “red pill” and “black pill.” Red pill narratives—popularised by figures such as Andrew Tate—suggest that self-improvement (via fitness, wealth, or confidence) can ‘rescue’ men from inceldom. In contrast, black pill thinking is more nihilistic, promoting the belief that no effort will ever overcome one's perceived undesirability. Unsurprisingly, the latter view fosters deeper despair and entrenched misogynistic and self-loathing thought patterns.
How Can We Support This Community?
A major takeaway from the session was the need to build trust, empathy, and non-judgement when working with incel-identified individuals. Person-centred approaches—such as Carl Rogers’ emphasis on unconditional positive regard—should be foundational before introducing more structured methods like Compassion-Focused Therapy (CFT) or schema therapy. These modalities can help challenge entrenched narratives of self-blame and rejection.
Crucially, therapists must avoid confrontational approaches, especially early in the therapeutic relationship. Labelling clients as misogynistic or attacking their worldview can prompt shutdown and resistance. Instead, we must approach with curiosity and compassion, creating a space where clients feel safe enough to explore and shift their perspectives.
Reflections on Digital Literacy
I found myself reflecting on my own digital identity. Though by age I may be considered a digital native or immigrant, I resonate more with the idea of being a digital nomad—someone constantly navigating unfamiliar digital landscapes. This talk reminded me how vital it is to deepen our digital literacy, especially as therapists. Online subcultures are shaping people’s self-concepts, and these virtual spaces must be accounted for in psychological formulation and intervention. Which i will talk about in another blog post.
A Special Thanks
Finally, I want to highlight the incredible contribution of the speaker from CEARs, a charity doing pivotal work in this area. Their expertise enriched the talk, and I highly recommend exploring their work if you’re interested in this topic.To learn more or engage with these themes further, visit:
email: enquiry@cear.uk
If you want to go to one of their amazing events by the Conn8cting- pub psychology community , follow the link below
https://chat.whatsapp.com/IBZS0yBYGdJIbLgZ21xc26
Lastly, Whilst reading this article, do any reflections or viewpoints come to mind?
Comment your views below.

My Journey to Becoming a Counselling Psychologist: Reflections So Far
It’s been a week since I received my acceptance letter for the Counselling Psychology Doctorate at City, University of London. It still feels surreal that I’ll be starting this September. Honestly, I cannot wait!
Now, I know exactly why I chose to become a counselling psychologist — but I also know there are tons of psychology-related professions out there. So, the purpose of this blog is to shed some light on the different psychological professions, whether you’re a psychology student figuring things out or someone looking to access support. But first... let me take you on a quick detour about how I even got to the point of applying.
The Origin Story
It all started back in college. I fell in love with A-level psychology (shout out to my psychology teacher who supported me during this time — you’re the real MVP!). Also, I was obsessed with Criminal Minds (P.S. I still am). The idea of analysing behaviour, understanding how thoughts and past experiences shape our actions — I was hooked.
Believe it or not, my original plan was to become a forensic psychologist. That dream pushed me toward a psychology undergraduate degree. By the time I wrapped up my undergraduate degree, I was convinced I’d pursue a Clinical Psychology Doctorate — because, let’s be honest, that’s all anyone on my course ever talked about. But then life (as it tends to do) gave me some perspective.
Through both personal experiences and professional roles, my understanding of what it means to be a clinical psychologist began to shift. I also discovered other doctorates — Counselling, Educational, Health Psychology, and more. Landing a job as a CBT therapist in a team filled with a wide range of psychological professionals was a game-changer. To be fully honest, before that role, I’d only ever worked with clinical and counselling psychologists. I’d never even heard of psychoanalytic psychotherapists or systemic therapists, let alone worked with them.
While working in that team, I attended a Counselling Skills Workshop at City. That experience lit a spark in me. I took a step back and started seriously researching the different psychological professions.
And let me tell you:
It can be super overwhelming — there are so many paths.
Some sources say different things about the same roles. (Confusing, right?)
So, to make life a little easier, I’ve pulled together a table that summaries the key differences between various psychological professions (based on my understanding).
Disclaimer:
These descriptions are my take on each profession. I absolutely welcome comments from people in the field — feel free to add anything I might have missed. It’ll help me (and others) keep learning!


So now reading into all the different professionals it made me realise that constant psychology is where I need to be. Lastly, whilst reading this blog, do any reflections or viewpoints come to mind?
Comment your views below

Cultural Adaptation in Therapy: Part 2
Welcome back to Part Two of our series on cultural adaptations in therapy. In this blog series, I'll summarize the talks and training I've attended, share my work experiences, and reflect on how these have enhanced my knowledge and skills for working in a culturally sensitive manner.
BABCP Event: Cultural Approaches in CBT
I attended a seminar facilitated by the BABCP on Cultural Approaches in CBT, which I believe applies to any psychological model or theory. The seminar covered the following topics:
The Needs of Racial Minority Communities and Existing Barriers
It was discussed that research supporting CBT as evidence-based often has fewer participants from racial minority backgrounds. Some studies do not state the ethnicity of participants, questioning the generalizability of results to all ethnicities.
Research showed that people identifying as White are more likely to improve or recover after IAPT psychological therapies compared to others.
Mental distress in the East is understood differently compared to the West, with spirituality and religion often playing a more significant role in support.
There is a need for more community collaboration and outreach in places of worship and linking up with religious leaders in clinical work.
Professionals and services may not seem competent or accessible to meet the needs of racial minority people. The following cultural barriers to therapy were discussed:
Mistrust of Service/Practitioner: Due to historical exploitation, such as the Tuskegee Syphilis Study and the Henrietta Lacks case, people from minority backgrounds often do not trust services/practitioners.
Lack of Understanding of Cultural Norms and Values by the Therapist
Fear of Stigmatization: Mental health is still heavily stigmatized in certain cultures (e.g., African culture). Clients may fear invalidation and ostracization for their difficulties.
Language and Terminology: Misunderstandings can arise from language barriers.
The link between racism, poverty, violence, and mental health is not often discussed in therapy. Clinicians need to consider how these factors affect clients daily and their environment. Trust and time are needed for clients to feel comfortable discussing these issues.
Assessment, Formulation, and Therapy Considerations Incorporating Aspects of Identity
During the talk, a case example was discussed, illustrating cultural adaptations at each point of the therapeutic process. Here are the key points:
Cultural Adaptations at Point of Referral:
Consider potential barriers to help.
Make services more accessible.
Understand the client's thoughts and feelings.
Reflect on your own thoughts and feelings, considering similarities and differences with the client and their impact on the therapeutic relationship.
Consider using a social identity map.
Cultural Adaptations in Assessment:
Gather background information from systems, other professionals, and referrers.
Offer the option of an interpreter if the client wishes and explain confidentiality.
Be flexible when contacting the client, considering the timing and frequency of appointments (e.g., avoiding clashes with prayer times or religious events).
Once trust is developed, ask about racism or other barriers to therapy, for example: "Is it okay for me to ask if you experienced racism in that situation?"
Cultural Adaptations in Formulation:
Collaboratively develop a shared formulation with the client, including their belief system in the 5 Ps formulation.
Explore differences between the client's home country and the current country, and how these differences contribute to their mental health condition.
Consider how the client's culture, ethnicity, social context, and identity, and their power in society, play into their current formulation.
Do not challenge or minimize a person's beliefs or viewpoints about their current concerns or experiences.

Cultural Adaptations in Intervention:
Explain concepts using the client's terminology. For example, if a client believes black magic is the cause of their mental health issues, explain how black magic may cause distress but is maintained and worsened by a vicious cycle, then explain the CBT cycle.
Integrate cultural support into therapeutic support, such as linking prayer with routines and self-care. Encourage clients to practice mindfulness and relaxation techniques after or during prayer.
Avoid pathologizing spirituality to prevent disengagement.
Respect for beliefs and values is central to engagement.
Values will include ideas about how one should act in various areas of life.
Short Guide to IAPT: BAME Service User Positive Practice Guide
Use a genogram that includes the migration histories of family members and discuss the degrees of acculturation of different family members to understand BAME service users' perspectives.
Develop community-specific steering groups, involve more people from BAME backgrounds in service user groups, and provide workshops in community settings and places of worship.
Use a recovery-based approach that incorporates the social, community, and spiritual needs of the service user.
Ensure therapy provision is available based on service user needs irrespective of their ethnicity, religion, or refugee status.
How This Information Will Influence My Practice:
Throughout the therapeutic process, I will keep in mind the barriers my clients may face in accessing services. I will take the time to build trust with clients before exploring these barriers. Here are some ways to do this:
Provide consistency in sessions.
Offer extended assessments, taking time to explore information with the client and build rapport.
Give clients time to talk through their concerns about therapy and the service.
I will consider the values and spiritual perspectives of service users throughout treatment, understanding that adaptation is essential on an individual basis—one size does not fit all. I will use supervision to support reflective practice and think about ways to adapt therapy. Utilizing resources or directories of organizations that offer support and advocacy will improve engagement in treatment.
I will also think about the practical side of therapy, such as if a client speaks another language or if English is not their first language, asking if they would like an interpreter, and actively listening to any concerns they may have around this. Additionally, I will remember that the same language can have different dialects, such as Bengali.
Even if there are similarities between me and the clients, I will explore the differences in our situations. Finally, I will consider my role and professional power, understanding that we have a duty of care for all clients. But do not worry, i will be reflecting on this last point in another blog.

Cultural Adaptions: Part 1
I work with diverse clients from various cultural, religious, social, economic and ethnic backgrounds. Due to this, I've been reading articles, attending talks and training around cultural competency, cultural adaptions to therapy and anti-racist practice to ensure better relationships with the clients I work with. This will
Ensure that clients feel respected and cared for throughout their time at the service.
Build a richer formulation of clients' needs and make sure their voices are heard throughout their time at the service.
Ensure that intervention best fits the client's needs, expectations and values.
I am also curious about cultural adaptations from assessment and intervention and how they may differ across different cultures. In this blog series, I will be summarising the talks and training I have attended during my work experience and reflecting on how these have enhanced my knowledge and skill set to work culturally sensitively.
Culturally Sensitive Assessment
This talk discussed how culture shapes mental health issues and the importance of cultural sensitivity in assessments. I was also trained in the Cultural Formulation Interview (CFI), a DSM5 tool traditionally used to ensure mental health diagnoses and interventions are more culturally sensitive. The Key Components of the CFI are below:
Cultural Definition of the Problem
In this section of the CFI, we will be trying to look for the following:
A person's way of understanding the problem.
How an individual frames their current problems to other members of the social network, i.e. families and friends.
Example Questions
People often understand their problems in their way, which may be like or different from how doctors describe the problem. How would you describe your problem?
Sometimes, people describe their problems differently to their family, friends, or community members. How would you describe your problem to them?
Cultural Perceptions of Cause, Context, and Support
In this section of the CFI, we will be trying to look for the following:
What the individual identifies is the cause of their problems.
For example, in some cultures, mental health is the result of bad things that happen in their life, problems with others, a physical illness or a spiritual reason.
The individual's life context focuses on resources, social support, and resilience.
I.e. from co-workers, from participation in religion or spirituality
Example Questions
What do you think are the causes of your problem? Is there any support that improves your situation, such as support from family, friends, or others?
What do others in your family, friends, or community think is causing your problem?
Do any aspects of your background or identity affect your problem?
Cultural Factors Affecting Self-Coping and Past Help-Seeking
In this section of the CFI, we will be trying to look for the following:
How does a person cope with their problem? What was/wasn't helpful? And why?
Either by medical care, mental health treatment, support groups, work-based counselling, folk healing, religious or spiritual counselling, or other forms of traditional or alternative healing
The role of social barriers to help-seeking, access to care, and problems engaging in previous treatment. (basically, what got in the way of them accessing help?)
For example, lack of money, work or family commitments, stigma or discrimination, or lack of services that understand your language or background?
Cultural Factors Affecting Current Help-Seeking
In this section of the CFI, we will be trying to look for the following:
An individual's current perceived needs and expectations of help.
The views of the social network regarding help-seeking.
Example Questions
What kind of help would be most helpful to you with your current problem?
Are there other kinds of help that your family, friends, or other people have suggested would be helpful for you now?
Cultural Factors in the Therapeutic Relationship.
In this section of the CFI, we will be trying to look for the following:
Any possible concerns about the clinician-patient relationship, including perceived racism, language barriers, or cultural differences that may undermine goodwill, communication, or care delivery.
Example Questions
Sometimes, doctors and patients misunderstand each other because they come from different backgrounds or have different expectations.
Have you been concerned about this, and can we do anything to provide you with the care you need?
How will this information influence my practice:
The CFI questions can easily be integrated into any initial assessment. The information from these questions could be used alongside any formulation model (such as the 5P's model) to develop a deeper understanding of a person's current concerns from an individual's and their network's social and cultural perspective. It will allow us to work holistically and identify areas of need.
Lastly, Whilst reading this article, do any reflections or viewpoints come to mind?
Comment your views below.

My Values: Part 1
So, I am starting a blog series about my work/life values, how they developed, and how they influence my practice. It's essential to know your values. When you're living and working inline with your values, it is a form of self-care. You're making sure your needs are being met.
I will not lie to you; identifying your core life values isn't easy. I feel like it taken me years to truly identified my values and going through the DClinPsy interview process helped me massively with this. I also want to make a disclaimer: our values are always changing. So my values now might be different in a few years, however, I will be talking about my values now. The first value I am going to talk about is Collaboration.
What is collaboration?
Collaboration can mean a lot of different things. However, for me it means working with two or more people or organizations to complete a task or achieve a goal.
How did I develop this value?
I first developed this value when I was younger. I was an undiagnosed dyslexic who struggled with reading and processing information throughout high school. To help me understand what I was learning and revise for exams (the task/goal), I would go around and discuss with other people who understood the topic and worked with them to support my understanding of a Topic. Furthermore, when I was struggling with managing my emotions, going to my close friends and talking it out with them always helped me manage my feelings and vice versa. These experiences have helped me develop the core belief/assumption that working with others is the best way to achieve a goal. I will use the CBT formulation below to explain these cycles.
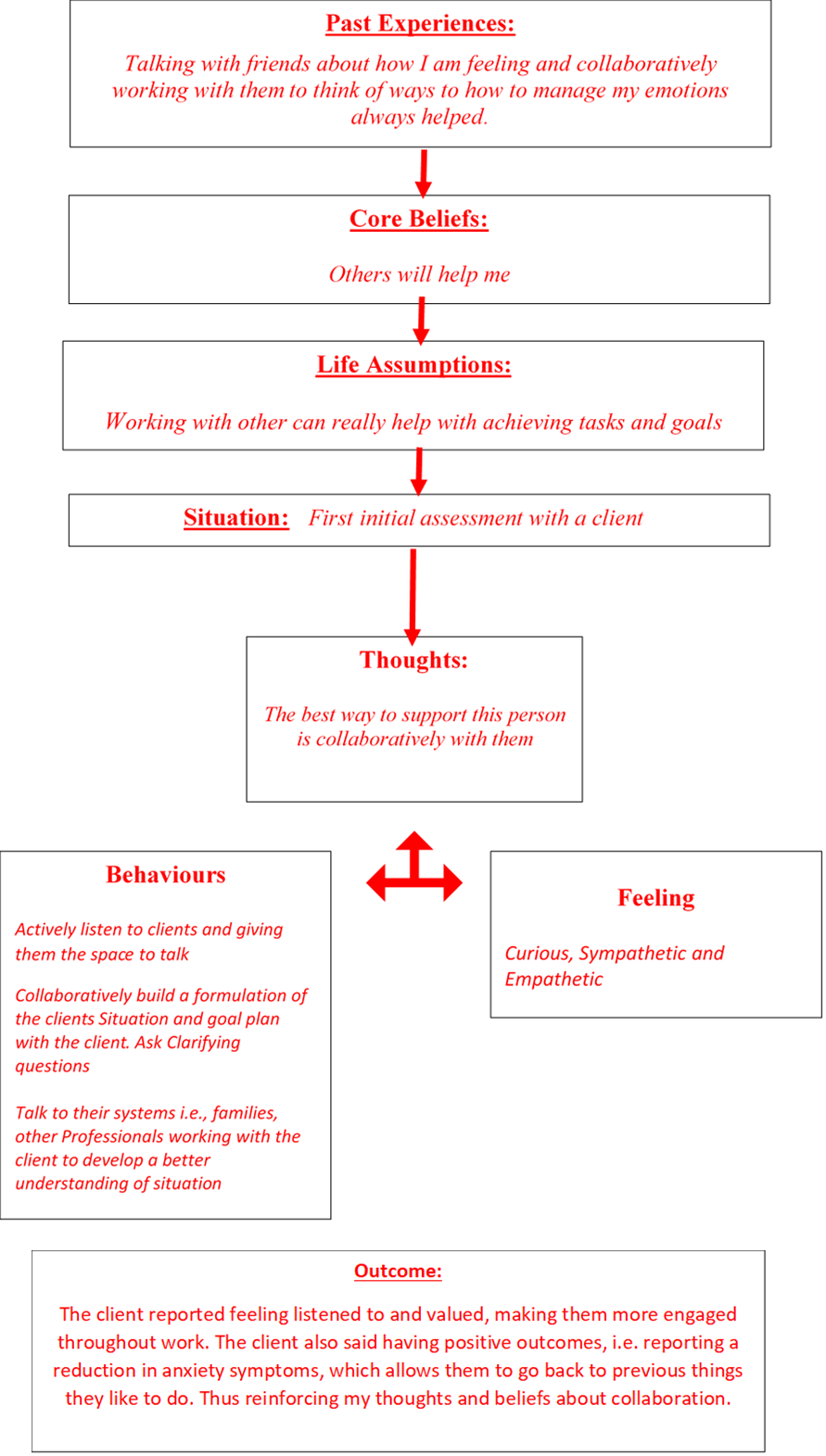
Whenever I worked collaboratively with the client, their network, and other local agencies to support their needs, I saw more long-lasting positive outcomes for the client. Conversely, when I haven't worked collaboratively with the client and have just been too focused on facilitating the therapy “correctly” due to my perfectionist tendencies, long-lasting positive outcomes aren't always achieved. (don’t worry; I will be talking about this in another article) These experiences have taught me the importance of involving clients and their networks at the centre of practice and the benefit it provides for clients in supporting their needs. This reflection is always in the back of my mind, providing me with the means to work with the mindset of putting clients at the forefront of my clinical practice.

Blog series: Psychological Therapies
Part 1 A: Cognitive Behavioural Therapy (CBT)
There are various psychological therapies that supports clients with various conditions. This blog series discusses their use in practice. This time around I'm focusing on CBT. CBT views mental health problems as exaggerations of normal processes, (the continuum principle) and focus on supporting current difficulties for effective therapy (the here-and-now principle).
Psychological Theory underpinning CBT
CBT is based on the two key theories:
Cognitive Theory
This theory states that our cognitions (our thoughts, mental images, beliefs and interpretations) about ourselves or an event or situation strongly influence our emotions and behaviours. (If you're still puzzled about what I am saying, don't worry, I will give you an example below)


An extra thing to add, Emotions cause bodily sensations to match the emotion, such as when relaxed, our body's heart rates lower, while anxiety causes uncomfortable feelings like stomach pains.
1) Behavioural Theory - Learning theory
This states that people acquire behaviours through environmental conditioning, affecting emotions and cognitions through actions. Basically, our behaviour or responses to our behaviour in a situation will change or maintain our emotions and cognitions.
For example, suppose you are person 1. Because of your anxiety, you start avoiding her and others due to worries about messing up in conversation and being called dull or stupid. Avoiding situations can provide relief from fear and reduce anxiety symptoms. However, continuous avoidance may lead to a false belief that anxiety symptoms are decreasing due to threats. You also don't get to discover if your thought is true, and you underestimate your ability to interact with others. The negative self-perception and the feeling that you learnt from your behaviours is how your behaviours maintain your anxiety.
CBT Model:
The model states that we develop core beliefs and assumptions which allow us to make sense of our world and find a way through it. As a result of our experiences, we create a range of functional and dysfunctional beliefs, with the functional ones allowing us to cope reasonably well most of the time.
However, when facing an event/multiple events that contradict our core beliefs or cannot be handled by our more helpful beliefs (sometimes called a critical incident), unhelpful assumptions can become active, triggering more unpleasant negative thoughts and emotional states like anxiety or depression.
The interactions between negative thoughts, emotions, behaviour and physiological changes may then result in persisting dysfunctional patterns, and we get locked into vicious cycles that maintain the problem (which I will refer to as maintaining processes later)

CBT formulation:
So not everyone knows what a “Formulation” is, so I will first explain what it is before going into the CBT formulation. In simple terms, a formulation is an understanding or hypothesis of a person’s current difficulties (don’t worry, I will do a whole separate blog on formulation because it is a big topic).
The CBT formulation uses the CBT model to develop:
· a description of the current problem(s);
· an account of why and how these problems might have developed;
· an analysis of the key maintaining processes hypothesised to keep the problems going.
Example of CBT Formulation:
This formulation below is an example of why a client has separation anxiety from their Mum

The key maintaining factors in this scenario are his negative thinking (worst-case scenario thinking), i.e. Mum is going to die when she leaves the house and the safety behaviours he does to manage his negative thoughts, i.e. Over texting/Calling Mum and Avoiding situations where he’s separating from Mum. This is because their Negative thoughts can increase their worry or fear, causing them to do Safety behaviours that stop them from directly testing their anxieties, and the untested fears will continue to arise in the future.
Assessment and Intervention in CBT:
When going through therapy in general there are 3 stages.
The Assessment stages
The Formulation stages
The Intervention stages
Throughout the Assessment stage of CBT, you and the clinician are building a formulation of your current problem. The treatment stage of CBT is supporting you to be your own therapist by helping you to understand and change maladaptive thinking and behaviour patterns by providing tools to change these patterns. (don’t worry again, in a separate mini-blog, I will explain some of the tools used).
So based on previous blogs, you can kind of guess what my stance on CBT is, but I thought I would just outline below the key pros and cons of CBT
CBT Pro’s
· It has scientifically been proven to be as effective as medication in treating some mental health disorders.
· It is an Evidenced –Based treatment for various ages and presentations. It is delivered in a short time compared to other talking therapies.
· The highly structured nature of CBT means it can be provided in different formats and manualised, including in groups, self-help books and computer programmes. It is also easy to train staff on this approach.
· The Skills you learn in CBT are useful, practical, and helpful strategies that can be incorporated into everyday life to help you cope better with future stresses and difficulties, even after the treatment has finished.
CBT Con’s
· CBT focuses on the individual's capacity to change themselves (their thoughts, feelings, and behaviours) and does not address wider problems in systems or families' relationships which can often significantly impact an individual's health and well-being.
· The model this therapy is based on was developed by a certain demographic of people - white, British, upper-middle-class male, and is this generalisable to everyone.
· CBT only addresses current problems and focuses on specific issues; it does not address the possible underlying causes of mental health conditions, such as an unhappy childhood.
· It involves confronting your emotions and anxieties; you may experience initial periods where you are more anxious or emotionally uncomfortable.
Lastly,
What are your reflections on this blog?
What your views about CBT?
Any questions you want answered?
Comment your views below

Other Points: Part 1
I didn't know what to label this article, so I just called it "Other Points" (Maybe someone can try and think of a name for it in the comments). I realised something while reading articles and talking to other colleagues at work, evidence-based psychological interventions, i.e., Cognitive Behavioural Therapy (CBT), the NHS provide, are based on research data and psychological theories representative of a demographic of individuals with similar cultural, religious, social, economic and ethnic backgrounds (Specifically, people from the white, middle-class upper class, males and the western world). This is know as the WEIRD problem in psychology.
I even remember discussing how assessment questions and diagnostic criteria is Westernised and how this could lead to information that might not accurately represent a client's difficulties (especially individuals from or brought up with the non-Western world, beliefs and values). See Scenario 1 & 2 below to see what I mean.
Scenario 1:
In most non-Western cultures, respect for your elders is a massive message taught (I was), and you are taught never to interrupt or answer back anyone older than you. So, as a parent from this culture (who has raised their child with the same value), You're in an ADHD assessment, and a clinician is trying to assess whether your child is impulsive (a diagnostic criterion for ADHD). The clinician asks you the standard question, "Does your child interrupt you or talk over teachers?" or "Do they blur out answers before questions have been completed?". They then follow this up with an example of whenever you talk to your child, does he interrupt you, or when he speaks to other adults, does he? Naturally, you will say no because your child has probably learnt that behaviour and is conditioned not to interrupt when an adult is talking and has never done it in Infront of you. This may cause the clinician to think there isn't any impulsivity and not ask follow-up questions.
But what if a different example was used. for example, does your child interrupt younger children when they talk, or their peers. The response might be different as your child may display their impulsivity in this way as its not deemed as culturally unacceptable to do this.
Scenario 2:
So, let's say you're a clinician conducting a child interview or observing a child at school for an Autism assessment, and you observe an ethnic minority child not providing eye contact with you or their teachers in the classroom. You might note that this is a behavioural sign of autism. However, in some non-Western cultures, especially African culture, giving direct eye contact to an elder is seen as disrespectful and rude. So, it would be essential to explore cultural upbringing with this child's family before saying that lack of eye contact is only explained by autism alone.
The above scenarios are just a few prominent examples of why It's important to hold cultural factors at the back of your mind throughout assessment, formulation and intervention, as they can impact the formulation of a client's needs. Now, coming back to my point about the NHS using evidence-based psychological interventions based on research data and psychological theories representative of a specific demographic of individuals. I completely get that they are evidence-based and have been shown to support various conditions. However, we wouldn’t prescribe medication for a condition where research only indicates it can help a specific demographic of individuals to every demographic with the condition. That would be unethical. To even have medication approved by the FDA, it must go through a series of drug trials, using participant from a range of different demographics.
So, why as psychologists do, we still worship CBT and other psychological therapies? I can't answer that question, but since they are the norm, what I can do is to provide cultural adaptions to the CBT/Psychological therapies assessment and intervention (Don’t worry, I will be going into this in another article).
Lastly,
What your reflections on this blog?
How do you adapt the therapeutic or diagnostic process to clients from different ethnic background?
What should I name the blog?
Comment your views below

The Big MAC event
The Big MAC event brings together lived experience experts and NHS professionals from various fields to discuss NHS service management, operational and strategic matters, and major developments in services and trust.
Overview of the Event
The challenges of working within the NHS
A consultant psychiatrist facilitated this part of the talk. There were discussions about the following:
Moral Injury and how NHS clinicians are working in an under-resourced system and then being abandoned to inevitable failure.
We talked about how systems are designed to exclude client and give any possible reason to keep people out. We talked about how services may not accept client based on the following:
postcode,
diagnosis,
complexity,
comorbidity.
Too much need or not enough need.
Too high Risk or for not being risky enough, lack of motivation,
A client's readiness for change
The language used in psychiatry (applicable to other professions, too) adds to the exclusion culture within NHS.
Professionals hear traumatic event from client they are working with, and this in-turn influences professional perceptions and beliefs of the world, leading to self-protection behaviours I.e., exclusion criteria.
How in only the pandemic has this been brought to light, and efforts have started to have been made towards supporting staff.
The use of terms such as "low risk" so we do not have to deal with it immediately, or they don't meet the criterion to access a service they need as the case is not "Complex enough."
How we continue to behave as if the risk is both predictable and quantifiable, using risk categorizations (low, medium, and high) even though this system is not evidence based.
The tendency to stray from objectivity into judgement in psychiatric notes. For example, using terms like 'manipulative' and 'behavioural' infer that a patient is doing something consciously and deliberately.
P.S. For more detailed information on the topics above, type the article "Magical Thinking and moral injury: exclusion culture in Psychiatry" into Google
The Impact of Moral Injury and Magical Thinking on Clinical Practice
Another consultant psychiatrist facilitated this part of the talk. There was a discussion about the following:
Exclusion in mental health is a long-standing concept, but it's just changed over the years and how excessively risk-averse and under-resourced system may drain its clinicians of compassion, losing sight of the human being behind each 'protected' bed and rejected referral.
In psychiatry, when professionals are distressed, clients are more likely to be looked at like scientific objects, which can lower the professional's ability to care for and be compassionate to clients.
How service could exclude via magical thinking (thinking that if we refer clients to another service that can offer more support, they will get help there). However, we need to realize they will sit on another year or months-long waiting list for this support.
Importance of organizations and services being able to support professionals even when in a distressing environment so that professionals can provide care not based on their superego.
The impact on Service user experiences of the NHS
A Service user facilitated this part of the talk. There was a discussion about the following:
Their diagnosis of borderline personality disorder (BPD) and the treatment they received in the NHS (known as MBT therapy), and how to benefit from the skills they were taught in this therapy.
They further discussed their experience with NHS services and barriers to obtaining support. These are listed below:
The impact of having the diagnosis and how, because BPD is still stigmatized, how professionals treat them differently because of their diagnosis
How medication is not always the answer to mental health conditions.
The assessment process can be challenging and make clients feel as though they must be assessed to see if they are good enough for services, and how professionals should always think of ways to reduce the power dynamic in the assessment phase.
How some people or clinicians see the behaviour but not the pain behind the behaviour.
Potential Solutions: What can we do next?
Realism and honesty should be embedded in the training rather than teaching perfect medicine in an imperfect world. The client will have more trust in us if we are open about the scarcity of resources and restrictions on referrals; if we acknowledge that we cannot provide all we would like to.
Being uncomfortable and having adequate Staffing support.
Meaningful training and service development should be truly involve service users throughout and how a fundamental problem is focusing on beds, breaches, and targets instead of the human story behind each number.
Organizations hierarchical changes.
Lastly, As the reader, what are your views:
Whilst reading this article, do any reflections or viewpoints come to your mind?
Do you agree or disagree with some of the points made?
Comment your views below.

“Superpowers, Strength and Neurodiversity”
What is Neurodiversity?
So, I realise that before I can write an article about Neurodiversity, I have to explain Neurodiversity.
Neurodiversity is used to describe a group of neurodivergent individuals who experience, process and interact with the world around them in many unique and different ways”.
Most common types of neurodiverse conditions are:
Autism, or Autism Spectrum Conditions.
ADHD: Attention Deficit Hyperactivity Disorder, or ADD: Attention Deficit Disorder.
Dyscalculia.
Dyslexia.
Dyspraxia, or Developmental Coordination Disorder (DCD)
DISCLAIMER : Neurodiversity is not a small topic and I would suggest you do some extra reading into it if you want to find out more as my explanation is a brief description.
My Diagnostic Experience
In 2020, I was diagnosed with Dyslexia. I remember the educational psychologist saying, “Wow, you are dyslexic; how come no one had picked this up throughout your education”. By the end of the week, I was given a 20-page dyslexia report highlighting all the support I would need at university, my dyslexia strengths, and difficulties and all the score of my assessment in technical terms and that's how I received my Dyslexia diagnosis.
Discovering My Neurodiversity
Since 2021, I've been on a journey to develop a better understanding of my Neurodiversity. I feel like I started this journey as a part of my role is to teach newly diagnosed Autistic and ADHD young people about what their neurodiversity condition, and it got me thinking, what does Dyslexia mean to me. So, my first instinct is to go to my 20-page dyslexia report.
Now, of course, this didn't go well. I spent 20 minutes rereading the first paragraph over and over, trying to understand it, which gave me a headache, and I just gave up. Ironic how they gave the dyslexic person a 20-page report and expected them to understand their diagnosis by doing the one thing they struggle with, reading. Recently, I have come across a Podcast series by Natalie Brooks called "Dyslexia in Adults" to support and educate people on the reality of Adult Dyslexia (P.S. this is a great series).
Should strength be referred to as “Superpowers” in?
Superpower is a term sometimes used to describe all the strengths of having any neurodiverse condition. You're probably thinking about what the strength/superpower are of having any neurodiversity conditions. Well, if you want to know what they are, the imagine in title page sums it up. Superpowers is even used in some research to quote neurodiverse strengths. So, I was shocked when Natalie said in the "Dyslexia in Adults, The Strengths" episode that she used to get frustrated when dyslexia was talked about as a gift/ superpower, and she never uses superpower to describe dyslexic strengths. She also said that she thinks we shouldn't just use celebrities that have the condition whilst teaching people about their condition (which I personally use in my session with young people) for the following reasons below;
Reason 1: It doesn't bring into the conversation that there is a more complicated story and real challenges with dyslexia.
Reason 2: It alienates people.
Reason 3: Discussing dyslexic strengths like a superpower sets the bar too high for people. It makes people think that they must change the world or something incredible for their strength to be authentic and substantive.
She talked about her strengths being in little moments, like a quick idea that she has or her ability to think of a solution straight after she notices a problem. She finished her point by saying we should discuss strengths using real-life examples and challenges.
Should strength be referred to as “Superpowers”: My View
When I finished listening to the episode, I started to think about whether I should be using the word "Superpowers", but at the same time, I didn't quite understand her view at first. However, after taking a step back, drinking a cup of tea and reflecting on it, I can see her viewpoint. I do believe that we should be discussing strengths using real-life examples whilst alongside challenges. To take it one step further, we should teach people how to see their challenges as strengths or even support them in using their strengths to help their challenges. However, it's vital that we still explain strengths as a superpower and even use celebrities when discussing diagnosis.
Reason One: A typical question that people have when they receive any diagnosis is, "How does it affect their future?" (I know I certainly did). Talking about a superpower and seeing celebrities who have the same condition and are thriving can be so inspiring and put any doubt at ease around the future.
Reason Two: It helps in reducing the negative stigma around the condition. The teachings we provide to clients around a new diagnosis are the same way they will explain their condition to others. So, describing it in terms of superpower and showing celebrities brings some positivity to the condition, and if they define it like this to other, those people are more likely to talk to others about this condition in the same positive light.
Reflections & Conclusion
Upon reflection, the key things I will be taking into my practice are...
When I am discussing a new Autism or ADHD diagnosis with a young person and their parent, I will both use superpowers and celebrities but also talk about the young person's real-life strengths alongside their challenges.
Apply the above for all client groups and new diagnoses.
Provide an extra individual session to the clients when given any new diagnosis and allow them to ask questions. This is because I know not all services offer this, and this is something I still am trying to find myself, with my dyslexia.
Lastly, As the reader, what are your views:
Should we be describing our strength as superpowers and showing celebrities' to newly diagnosed clients or use using real-life examples of strength alongside challenges?
Should we do both?
How would you like a professional to explain to you about a new diagnosis you have?
Comment your views below